Case Presentation
History taken from Patient and Attendant (elder brother); Reliability 9/10.
A 49 year old English and Telugu language lecturer presented with a 2 month history of progressive asymmetric involuntary movements of his right index and middle fingers.
Present Illness
The patient reports that he first noticed them happening nearly 6 months ago, which was very small in amplitude, affecting these two fingers only. He says that these movements often worsened with rest and abated with activity. They were not troublesome initially but for the past 2 months he has been unable to correct answer sheets because of the involvement of his thumb and maintaining stability of his hand was proving difficult. He describes these movements as involuntary, rhythmic to and fro oscillations.
He also adds that his handwriting has become ugly with very small letters. On interviewing further, the patient reports that he feels stiffness in his wrists (Right>Left), which has now ascended to his elbows. He says the stiffness is present throughout the range of motion. He also says that since the last 1 month, the same involuntary movements also started appearing in his left hand.
At this point, he also says that his walking has become difficult with small, short steps and a forward stoop, and he feels that although he weighs 60 kgs. he feels like it weighs 100 kgs.
He does not report any difficulty in reading the newspaper, holding the paper, turning pages or folding it back. He does not have any difficulty in brushing his teeth or combing his hair. He also denies having difficulty in holding objects, such as holding a water bottle to drink nor any difficulty in mixing food and eating it. He does not have any difficulty in wearing a vest or in buttoning or unbuttoning his shirt. No difficulty in lifting his lower limbs and wearing a trouser.
The interview continues and we question for any difficulty in taking the stairs - he reports that he has been having difficulty in taking stairs up, in that he feels he sometimes might lose balance. He has no difficulty in descending stairs. The patient also denies having swaying of his trunk while walking or overshooting his hand while picking up objects.
On pressing further - he reports that he hasn't been having morning erections since 2 months and also reports a loss of sexual desire. He also says that since 2 months his bowel habits have been incredibly erratic, in that he sometimes has an immediate urge to defecate when he has tea and sometimes goes 2 to 3 days with constipation.
He, however, denies feeling dizzy or lightheaded when waking up in the morning. He denies having stiffness in his lower limbs, denies cotton wool sensation of floor, denies burning pain or inability to feel hot or cold stimuli. He also denies buckling of knees but, however, he reports that he has been having a great difficulty to walk in the dark since 2 months and says that he feels like he would definitely fall without support.
His brother gives a positive affirmation for all his symptoms and also says that he previously used to be a fairly jovial and hardworking man with good oratory skills, however, since the last 2 months he says his brother's speech lacks that 'edge' which he previously had. On asking further, the brother says that he has been speaking in a monotonous drab since 2 months.
The patient and his brother deny noting any fluctuations in his alertness, apathy or emotional instability to family or personal issues, no history of visual hallucinations, no history of incoherence of speech or irrelevant talk and no history of difficulty in managing finances or poor self care.
The patient denies ever having urinary incontinence, memory deficits, the brother vehemently denies the patient ever being anti-social, he does not have any difficulty in forming new memories or any visual deficits.
Past History
No similar complaints in the past. No history of Diabetes, Hypertension, Coronary Artery Disease, Seizures, Asthma or Tuberculosis.
Medical/Surgical History
The patient is not on any medications. He also did not report usage of any herbal or alternative medicine. He has no past surgical history.
Personal History
The patient is a teacher; he teaches English and Telugu for B.com and B.sc students in a college in Miriyalguda. He has been in this profession for the last 9 years. He has a triple M.A. in English, Sanskrit and Telugu.
The patient neither smokes nor drinks, he had a fairly routine lifestyle with waking up early in the morning and getting ready for his job. However since the lockdown, he had to stay at home with his college shut. He spends most of his time reading the newspaper and other literature. He lives with his wife and one son, who is studying Inter 2nd year. His sleep habits are well maintained. However, his bowel habits have changed in the last 2 months as detailed above. His appetite is good, he consumes vegetarian food on most days with a good access to nutritious food and clean drinking water. He occasionally enjoys non vegetarian food. He socialises well with his extended family and his local community. He is well respected among his peers and students alike.
Family History
No significant family history reported.
Social & Educational History
Married for 24 years with 1 child. Triple degree in MA in English, Sanskrit and Telugu.
Immunization History
Complete upto age 5.
General Examination
Patient is conscious, coherent & cooperative.
Vitals at the time of history taking -
PR - 88 bpm
BP - 190/110 mm Hg
After standing for 3 mins - BP - 160/110 mm Hg
Temp - Afebrile
RR - 16 cpm
No signs of Pallor, Icterus, Cyanosis, Clubbing, Generalized lymphadenopathy or edema.
Nervous System Examination
Higher Mental Functions
1. Level of consciousness - Normal (GCS 15/15)
2. Attention - Intact
3. Orientation - to time, place and person - Intact
4. Language - fluency & latency, comprehension, repetition, naming, reading and writing - Intact. Prosody - impaired
5. Memory - immediate recall, recent and remote - Intact
6. Other higher mental functions - general knowledge, abstraction, judgement, insight and reasoning - Intact.
MMSE
29/30 (No cognitive impairment)
CN Examination
1st
Normal (smell of soap).
2nd
Counting fingers at 6mts both eyes normal.
3rd,4th,6th
Pupil size. N N
DLR/CLR. N. N
No pstosis, nystagmus.
5th
Both sensory & motor normal.
Corneal & Conjunctival reflex +.
7th
Nasolabial fold normal.
No deviation of mouth.
Salivation & Lacrimation unaffected.
8th
Rinne's AC>BC.
Weber's - No lateralization.
9 th, 10th &
Palatal movements normal.
No difficulty in swallowing.
Gag reflex present.
11th
Movements of neck in all directions+.
Lifting of shoulders +.
12th
Tone of tongue - Normal.
No wasting, no fibrillations & deviation of tongue.
Tongue tremor+.
MOTOR SYSTEM
Right. Left
✓Bulk Normal Normal
✓Tone
Upper limb R. L
Shoulder Normal Normal
Elbow Normal Normal
Wrist Hypertonia Normal
(Cog wheel rigidity)
Lower limb Normal Normal
✓Power
UL
Proximal 5/5 5/5
Distal 5/5 5/5
LL
Proximal 4/5 4/5
Distal 5/5 5/5
✓Reflexes
Superficial reflexes
Right Left
Corneal + +
Conjunctival + -
Abdominal + -
Plantar - -
Deep tendon reflexes
Right Left
Biceps 2+ 2+
Triceps 2+ 1+
Supinator 1+ Absent
Knee 3+ 3+
Ankle 1+ 1+
Clonus Absent. Absent
Involuntary movements - Resting tremors of Right upper limb , 3-4Hz, high amplitude.
Gait - Reduced arm swing.
Finger tap and toe tap - Normal.
No decrease in speed on repeating the movement continuously.
✓SENSORY SYSTEM
Right Left
Pain + +
Fine touch + +
Temperature + +
Vibration
Medial malleolus 5.7s 4.6s
Patella 9s 4.3s
Elbow 4.8s 6.4s
Wrist 5s 7s
Proprioception Normal Normal
Stereognosis Normal Normal
✓CEREBELLUM
Titubation - absent
HINTS
Head Impulse - negative
Nystagmus - negative
Test for skew - negative
Gait Ataxia absent.
Dysarthria absent.
Rebound phenomenon absent.
Intentional tremors - absent.
Pendular knee jerk - absent.
Tandem walking normal.
Coordination tests
Dysdiadochokinesia absent
Finger nose test normal
Heel knee test normal
Rombergs Test - Negative
Micrographia +
✓Findings - The movements in the right lower limb is slower than the movements in the left lower limb.
✓The first test was only toe tapping, the second test is entire foot tapping.
Rapid supination and pronation - Diadochokinesia
✓MENINGEAL SIGNS
Neck stiffness - Absent
Kernig's sign - Negative
Brudzinski's sign - Negative
✓AUTONOMIC
Postural hypotension+(Supine - 180/110, Standing 160/90).
Resting tachycardia absent(PR 80/min,regular)
Abnormal sweating absent.
H/O erectile dysfunction+.
Cardiovascular System
S1, S2 +.
Apex beat in 5th ICS on the MCL.
JVP normal.

✓ Shows Sinus Tachycardia with pseudo infarct pattern in leads I and aVL with dagger q waves in the same leads.
✓ No late intrinsicoid deflection of R wave with modified Cornell criteria showing LVH.
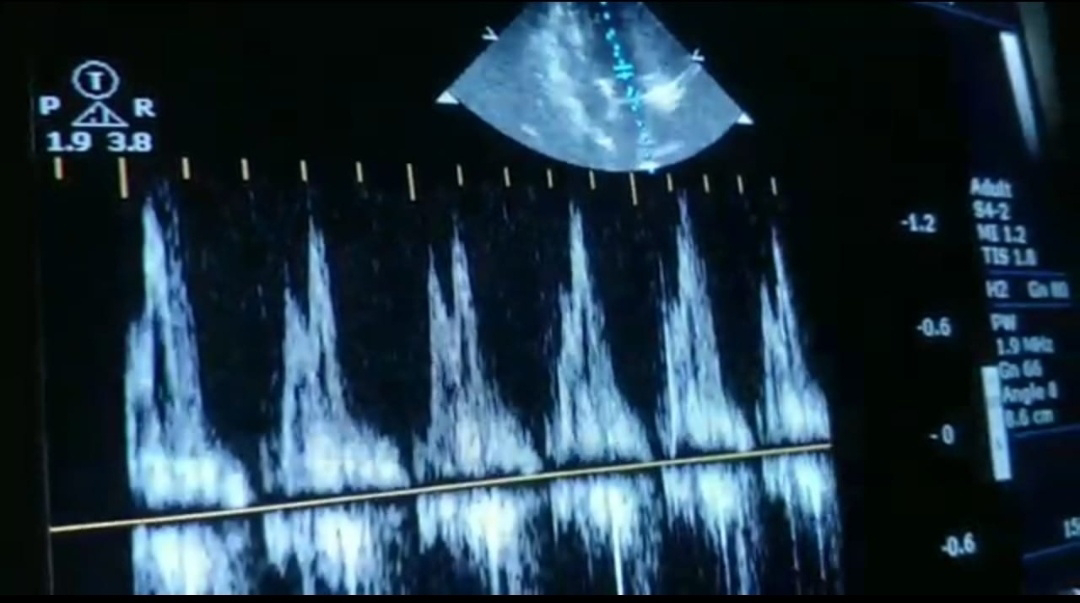
2 D Echo
✓ Grade II diastolic dysfunction.
Respiratory System
Shape & symmetry of chest - Normal
Respiratory movements - Equal on both sides
BAE+
NVBS
Abdominal Examination
Soft, Non-tender
No organomegaly
Bowel sounds+
Problem Representation -
A middle aged man presenting with a 6 months history of gradually progressive, asymmetric rest tremor with autonomic features is provisionally diagnosed with
1. Idiopathic Parkinson's Disease Stage 1 with denovo HTN.
2. Multiple System Atrophy - Parkinsonian Type (MSA-P).
Treatment
1. Tab. Syndopa Plus 125 mg QID
2. Tab. Syndopa 125 mg CR OD
3. Tab. Telma 40 mg OD
Sourced From - Resting Tremor (sravyakandala.blogspot.com)
Comments
Post a Comment
Your inputs are welcome :)